

Background: Bruton tyrosine kinase (BTK) inhibitors are effective treatments for B-cell malignancies, but an increased incidence of cardiovascular (CV) toxicities has been observed with ibrutinib. Acalabrutinib (acala) is a next-generation, potent, highly selective, covalent BTK inhibitor approved for chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma and mantle cell lymphoma. The objective of this analysis was to characterize CV adverse events (AEs) in patients (pts) with CLL who received acala monotherapy.
Methods: Data from pts with CLL in 4 studies (ACE-CL-001 [NCT02029443]; ACE-CL-007 [ELEVATE-TN, NCT02475681]; ACE-CL-309 [ASCEND, NCT02970318]; 15-H-0016 [NCT02337829]) were pooled. Cutoff dates ranged from December 2018 to February 2019. Pts who received ≥1 dose of acala monotherapy were included. For pts who crossed over from control arms to acala, only AEs recorded after crossover were included. Acala was given orally at total daily doses of 100 mg to 400 mg, later switched to 100 mg twice daily, and continued until disease progression (PD) or toxicity. Cardiac AEs and hypertension (htn) were examined.
Results: 762 pts were included (treatment-naïve: n=352 [46%]; relapsed/refractory: n=410 [54%]; median age: 67 years [range: 32-89]; Eastern Cooperative Oncology Group performance status ≤1: 93%; median acala exposure: 24.9 mo [range: 0-58.5]; median follow-up: 25.9 mo [range: 0-58.5]). A total of 199 cardiac AEs of any grade (irrespective of treatment relationship) were reported in 129 pts (17%). Cardiac AEs led to treatment discontinuation in 7 pts (0.9%). The most frequent cardiac AEs reported in ≥2% of pts were atrial fibrillation (afib: n=34; 4%; afib/flutter: n=38; 5%), palpitations (n=23; 3%), and tachycardia (n=17; 2%). The median time to afib/flutter onset was 521 days (range: 8-1280). Overall, 91% (117/129) of pts with vs 79% (503/633) without cardiac AEs had ≥1 CV risk factor before acala initiation. The most prevalent CV risk factors (≥20%) among the 129 pts with cardiac AEs were htn (n=86; 67%), hyperlipidemia (n=38; 29%), and arrhythmias (n=29; 22% [afib: n=16; 12%]). Htn AEs were reported in 9% (67/762) of pts, among whom 46 (69%) had pre-existing htn and 18 (27%) had htn risk factors. The median time to htn onset was 197 days (range: 2-1345).
Thirty-seven pts (4%) had 51 grade ≥3 cardiac AEs (grade 3: n=37; grade 4: n=12; grade 5: n=2). Grade ≥3 cardiac AEs of interest included afib (n=10; 1.3%), complete atrioventricular (AV) block (n=2; 0.3%), acute coronary syndrome (n=1; 0.1%), atrial flutter (n=1; 0.1%), second degree AV block (n=1; 0.1%), and ventricular fibrillation (n=1; 0.1%). Two patients experienced grade 5 AEs (cardiac failure congestive [n=1], acute myocardial infarction [n=1]). Among the 37 pts with grade ≥3 AEs, 18 (49%) were continuing acala at data cutoff; 6 (16%) had discontinued due to the grade ≥3 cardiac AEs, 4 (11%) to other AEs, 5 (14%) to PD, 3 (8%) to death, and 1 (3%) to other reasons. Among the 51 grade ≥3 cardiac AEs, 16 (31%) led to dose delay and 36 (71%) were managed with concomitant medications. Most events (43/51 [84%]) resolved (dose delay: n=15; drug withdrawal: n=4; no dose change: n=24).
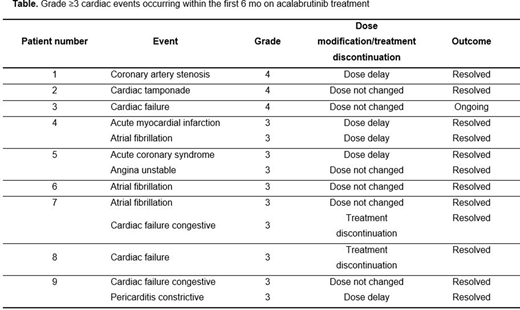
Cardiac AEs occurring in the first 6 mo on acala were assessed based on a predominance of AEs (afib) during this time period with ibrutinib (Brown JR, et al, Haematologica. 2017;102:1796). Overall, 48% of pts with any-grade cardiac AEs experienced them in the first 6 mo on acala. Thirteen grade ≥3 cardiac AEs (25% of total) were observed in 9 pts in the first 6 mo (Table); all but 1 AE (grade 4 cardiac tamponade resulting in hospitalization) were managed with concomitant medications. Two of the 13 AEs resulted in treatment discontinuation (Table).
Conclusions: At a median exposure of 24.9 mo, cardiac AEs occurred infrequently in pts with CLL treated with acala monotherapy; only 0.9% discontinued treatment due to cardiac AEs. Among grade ≥3 cardiac AEs, 25% were reported during the first 6 mo on treatment. Most pts with cardiac AEs had pre-existing risk factors that may have contributed to their development. The incidence of afib with acala (4%) was comparable to that of the general CLL population (6.1%; Shanafelt TD, et al. Leuk Lymphoma. 2017;58:1630). These data suggest a low risk of cardiac AEs with acala treatment in pts with CLL. The safety of acala vs ibrutinib in pts with high-risk CLL will be investigated in the phase 3, randomized ACE-CL-006 trial (NCT02477696).
Brown:Janssen, Teva: Speakers Bureau; Abbvie, Acerta, AstraZeneca, Beigene, Invectys, Juno/Celgene, Kite, Morphosys, Novartis, Octapharma, Pharmacyclics, Sunesis, TG Therapeutics, Verastem: Consultancy; Gilead, Loxo, Sun, Verastem: Research Funding. Byrd:Acerta Pharma: Research Funding; Syndax: Research Funding; Leukemia and Lymphoma Society: Other; Trillium: Research Funding; Kartos Therapeutics: Research Funding; Vincera: Research Funding; Novartis: Research Funding; Janssen: Consultancy; Pharmacyclics LLC, an AbbVie Company, Gilead, TG Therapeutics, BeiGene: Research Funding; Pharmacyclics LLC, an AbbVie Company, Gilead, TG Therapeutics, Novartis, Janssen: Speakers Bureau; Pharmacyclics LLC, an AbbVie Company, Janssen, Novartis, Gilead, TG Therapeutics: Other. Ghia:Adaptive, Dynamo: Consultancy, Honoraria; Novartis: Research Funding; Acerta/AstraZeneca: Consultancy, Honoraria; ArQule: Consultancy, Honoraria; Gilead: Consultancy, Honoraria, Research Funding; BeiGene: Consultancy, Honoraria; Janssen: Consultancy, Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company), Research Funding; Celgene/Juno: Consultancy, Honoraria; Lilly: Consultancy, Honoraria; MEI: Consultancy, Honoraria; Sunesis: Consultancy, Honoraria, Research Funding; AbbVie: Consultancy, Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company), Research Funding. Sharman:TG Therapeutics: Consultancy, Research Funding; AbbVie: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Pharmacyclics: Consultancy, Research Funding; AstraZeneca: Consultancy, Research Funding; Genentech: Consultancy, Research Funding; Acerta: Consultancy, Research Funding; Roche: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Bristol Meyers Squibb: Consultancy, Research Funding; BeiGene: Research Funding. Hillmen:F. Hoffmann-La Roche: Honoraria, Research Funding; Astra Zeneca: Honoraria; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company), Research Funding, Speakers Bureau; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company), Research Funding, Speakers Bureau; Pharmacyclics: Research Funding; Gilead: Research Funding. Stephens:MingSight: Research Funding; Acerta: Research Funding; Karyopharm: Consultancy, Research Funding; Gilead: Research Funding; Arqule: Research Funding; Pharmacyclics: Consultancy; Verastem: Research Funding; Beigene: Consultancy; Juno: Research Funding; Innate: Consultancy; Janssen: Consultancy. Sun:VERASTEM, GENMAB: Research Funding. Jurczak:Janssen, MeiPharma, Merck, Pharmacyclics, Roche, Tekeda, TG Therapeutics: Research Funding; Maria Sklodowska-Curie National Research Institute of Oncology: Consultancy, Current Employment; Jagiellonian University: Ended employment in the past 24 months, Research Funding. Patel:AstraZeneca: Current Employment, Current equity holder in publicly-traded company. Baek:Acerta Pharma: Current Employment. Lezhava:Astra Zeneca: Current Employment; Melinta Therapeutics Inc: Ended employment in the past 24 months. Kuptsova-Clarkson:AstraZeneca: Current Employment. Moslehi:AstraZeneca, Janssen, BMS, Boston Biomedical, Immunocure, Myovant, Boston Biomedical, Deciphera: Consultancy. Furman:Acerta: Consultancy; Abbvie: Consultancy; Verastem: Consultancy; Sunesis: Consultancy; Pharmacyclics: Consultancy; Oncotarget: Consultancy; Loxo Oncology: Consultancy; Janssen: Consultancy, Speakers Bureau; Incyte: Consultancy; TG Therapeutics: Consultancy, Research Funding; AstraZeneca: Consultancy, Research Funding; Beigene: Consultancy; Genentech: Consultancy.

